here's a video of a talk i gave a couple of weeks back at Addictions Rounds to an audience of clinicians/treatment providers and researchers:
"Addiction Neuroimaging: What is known, and (how) can it be used?"
unfortunately the beginning got cut off. missing slides after the jump.
First I’m going to spend some time talking
about addiction and the brain, then give an overview of some of the most common
neuroimaging techniques, and then discuss some skillful and unskillful uses of
these techniques in the field of addiction. After that, I would like to talk to you about some ways that
this type of knowledge can be useful for practice, and give one example, which
is my pitch for therapeutic patient education in addiction. Finally, I would love to have a
discussion about other ways, and hear from you what you feel is needed and how
neuroimaging knowledge can be leveraged to improve clinical practice.
Starting with addiction and the brain, I
would like to point a quote I once heard, that the mind
is what the brain
does. Most people would agree that
the two are inextricably linked, and that without the brain, there can be no
mind. As such, since addiction is
thought of as a mental condition, part of our understanding of the condition
has to come from understanding the brain. The reason I am pointing out what seems
obvious is that different people conceptualize addiction in different
ways. This includes the disease
model, but there are some schools of thought where social, environmental, psychological,
and historical variables play a bigger part. My opinion is that these views are not necessarily
incompatible, because they all somehow link back to some kind of
neurobiological process that ultimately steers a person’s behaviour – although
it could be that we know nothing about that process. If you believe that there are
neurobiological underpinnings to addiction, then neuroimaging is a powerful
tool in helping us understand. For
one, it helps understand the
human experience, rather than mice or cell
cultures or test tubes, and also, it helps develop biomarkers, which are
biological intermediaries between internal/
or external processes and behavioural outcomes, and as such, have the advantage of being objective. People’s internal and external experiences, self-reports,
etc are so varied that it is difficult to find commonalities, so imaging
provides some standardized measures that can then be compared across people and
tested for utility moving forward.
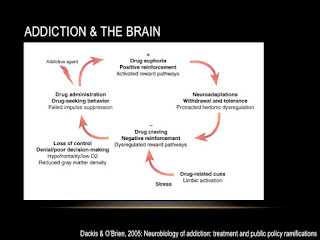
This is one way in which addiction and the
brain can be conceptualized. The
first thing you’ll notice is that it isn’t a unitary construct, but rather,
made up of a number of nodes that are arranged in a cycle. These begin with administration of the
addictive agent, which produces euphoria and reinforcement, which, with
repeated administrations, result in neuroadaptations underlying processes like
withdrawal and tolerance. If you
now add emotional components to the mix, like drug cues or stress, the result
will be drug craving, eventually leading loss of control and poor decision making,
and ultimately drug seeking and administration, starting the cycle all over
again. You can see on here that each of these
components is associated with certain neurobiological correlates, and the field has made great strides in
understanding those correlates, using neuroimaging. The reason this is important is that each of the nodes can
be a target for intervention, but requires a thorough understanding first.



No comments:
Post a Comment